



Discuss your application with an expert
How do you investigate the mechanisms of pulmonary infection?
There is an increasing emergence of previously unknown pathogens and antimicrobial resistance causing pulmonary infection. The COVID-19 pandemic was an exemplar of the requirement for new approaches that facilitate a rapid understanding of and therapeutic design against novel pathogens.
The lung is the only internal organ directly subject to the environment and is therefore particularly vulnerable to pathogens. This, together with the increasing emergence of novel pathogens and antimicrobial resistance, has caused lower pulmonary infections to become a leading cause of death worldwide.
However, the likelihood of new pulmonary infection therapeutics reaching the market is only 3% compared to 6-14% for other disease therapeutics. This extremely high attrition rate can be partly attributed to the lack of reliable, predictive preclinical models that capture the intricacies of the human lung.
Our solution
Our two perfused multi-cell type Lung-on-a-chip (alveolar and bronchial airway) models map the distinct physiology of the human lung, making it possible to study the mechanism of pulmonary infection, drug responses, host-pathogen interactions, and immune response.
Our models show improved differentiation of alveolar and bronchial cells into physiologically relevant phenotypes that provide superior tissue formation and differentiation into key cell types found in the human lung.
PhysioMimix® Pulmonary infection assays enable studies of the upper or lower airways. Co-cultures of epithelial and endothelial cells (with the potential to add multiple immune cell populations, including recirculating immune cells) accurately recapitulate the viral life cycle and host response.
The benefits
Map distinct pulmonary responses
Map and predict distinct physiologically relevant human responses to pulmonary infections by using and comparing the alveolar and bronchial lung-on-a-chip models.
Gain deeper insights
More sensitively determine inflammatory responses, tissue alterations and damage markers through multiple analyses of the large tissue and media volumes over infection periods and drug dosing.


This application was developed using funding from Innovate UK
Studying pulmonary infection
Limitations with current techniques
- The lung physiology and immunology of animal models differs from humans
- Inability to track specific immune responses to pathogens
- Simple cell models (e.g. VeroE6) only model virus entry and replication
- Animals are needed to look at the systemic effects of infection
Advancements with PhysioMimix Core
- Our lung models infected by pathogens produce physiologically relevant human inflammatory responses for therapeutic testing
- Complex co-culture provides phenotypes that reflect human physiology and immunology
- Gain insight into how different areas of the lung respond to pathogens.
- Ability to add multiple human immune cells (tissue-specific and circulating)
- Understand with high sensitivity the biology and immunology of pulmonary infection in humans
- Lung models can be connected to the liver to study multi-organ effects
End point measurements
Longitudinal and endpoint measurements include but not limited to:
Functionality biomarkers
- Production of mucus (bronchial model)
- Alcian blue – histology or colorimetric assay
- Production of surfactant (alveolar model)
- qPCR
Profiling analysis
- Barrier integrity (TEER)
- Epithelial cellular composition
- Microscopy or qPCR
- Lactose dehydrogenase (LDH) release
- Adenosine Triphosphate (ATP)
- Inflammatory response profiling
- Cytokine & chemokine immunoassays
- Confocal microscopy
- Transcriptomics
- Cellular phenotypes
- Viral receptor expression
- Genetic perturbations
Infection biomarkers
- Quantification of viral antigen
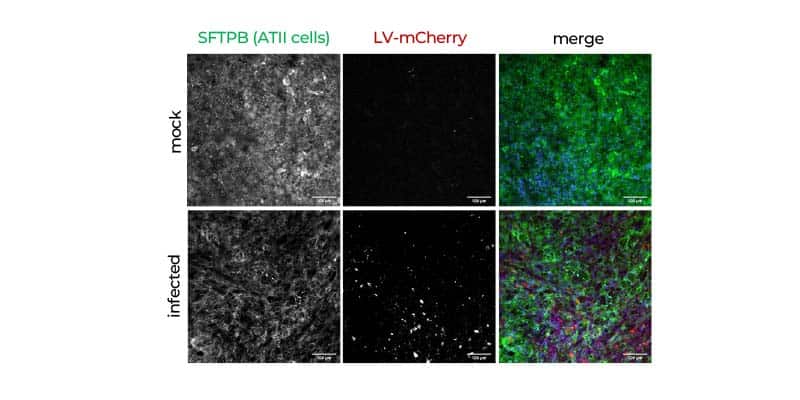
- Confocal microscopy immunofluorescence staining
- qPCR
- Transcriptomics
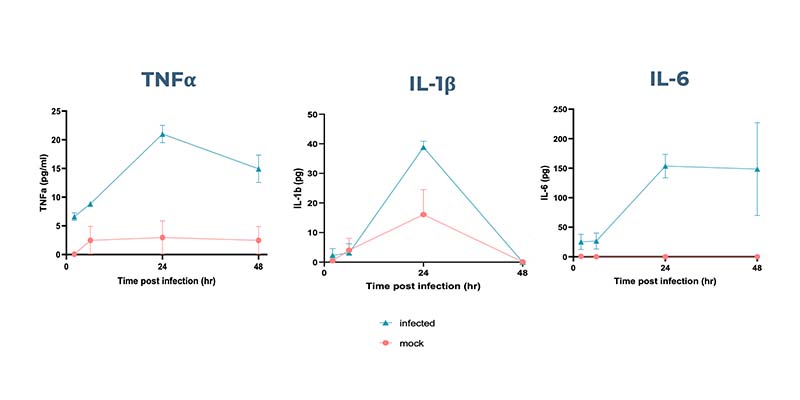
Human-relevant immune responses mapped over time
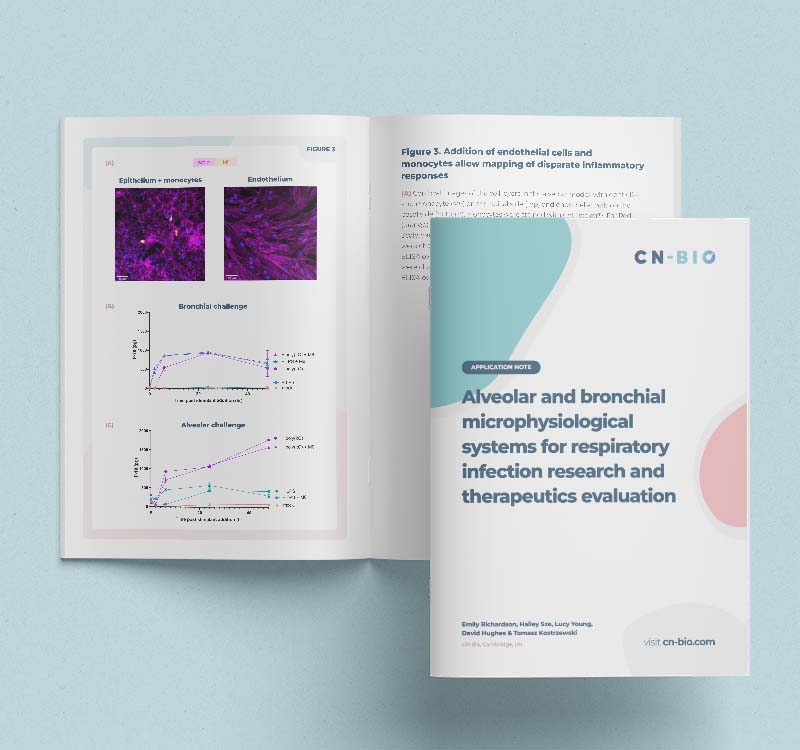
The inflammatory responses of alveolar Lung-on-a-chip models following infection by pseudotyped lentivirus expressing SARS-CoV-2 Spike protein demonstrate physiological relevance.
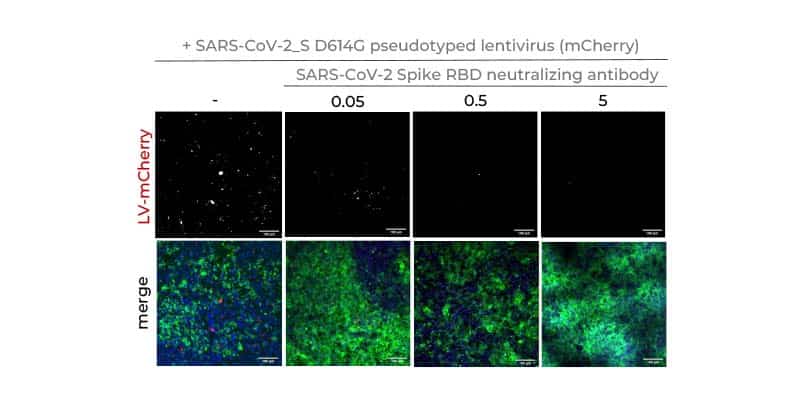
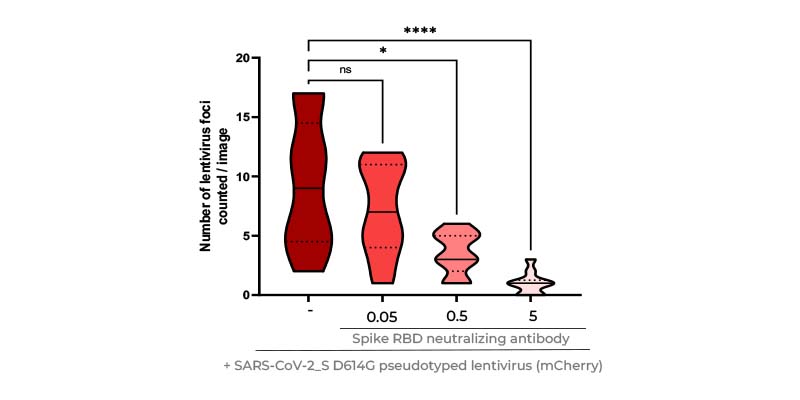
Rapidly determine the efficacy of novel therapeutics
Assess the ability of drugs to inhibit the infection of cells or to decrease inflammatory responses.
Predicting efficacy: COVID-19 Application Note
This application note demonstrates the model’s ability to predict therapeutic efficacy against SARS-CoV-2 and to facilitate an understanding of COVID-19 disease progression.
Explore our Lung-on-a-chip models
Recreate the airway or alveolar niche by culturing epithelial and endothelial cells on each side of an insert at ALI. Achieve a human-relevant barrier with enhanced functionality for longer term culture.
Add PhysioMimix Core into your lab
Harness the power of PhysioMimix OOC in your own lab. With a growing community of users and support from our experts, there has never been a better time to transition into 3D cell culture.
Frequently asked questions
What types of cells are used in your pulmonary infection assays?
For the lung models, we use primary pulmonary cells. In both alveolar and bronchial models, a combination of epithelial and endothelial cells can be cocultured on the apical and basolateral side of an insert, respectively. In our alveolar MPS model, commercially available small airway epithelial cells (SAEC) are used. In the bronchial MPS model, commercially available bronchial epithelial cells are used (NHBE). Both models can have the inclusion of pulmonary endothelial cells (HPMEC), which again are commercially available. We have also shown that immune cells can be included in the models, but do not have commercially available protocols for this – yet! Watch this space…!
View our Lung-on-a-chip page for more info
How many readouts can you get from your pulmonary infection assay over time and at endpoint?
The PhysioMimix Multi-chip Barrier plate contains 600 uL of media in each of 12 wells. In theory, the whole volume can be extracted for analysis per time point, or a smaller volume can be taken. This can allow a range of analyses to be made – from simple LDH measurements for cell health to multiple cytokine measurements. Media samples can be taken at any point during the experiment due to the open-well format of the MPS plate. The inserts can also be removed during experiments into a 24-well plate to visualize tissue changes. At the end of the experiment, the lung tissue can be analyzed in many ways, from high-content microscopy to genetic or –OMICs analysis by cutting the insert scaffold and extracting tissue. Together, these temporal, data-rich analyses can be used to build a high-resolution picture of lung-pathogen interactions.
In your pulmonary infection assays, how do you infect lung-on-a-chip models?
The lung-on-a-chip models are cultured on inserts, such as Transwells®. During differentiation and culture, the cells remain in an air-liquid-interface (ALI), where the apical side of the culture is subject to the air. For infections, small volumes of pathogen can be added to the apical side if recapitulating a pulmonary infection. If simulating a systemic infection, pathogen can be added to the basolateral side of the well. If a researcher wishes to stimulate an aerosolized dose of pathogen, the inserts can be removed from the Barrier-12 plate and placed in commercially available aerosolization chambers.
Why use lung-on-a-chip models for pulmonary infection studies rather than standard 2D / ALI / 3D spheroid models?
Through comparison of tissue phenotypes, we have noted that our lung-on-a-chip models have an enhanced human tissue phenotype both in terms of cell type expression and tissue architecture. For example, our alveolar MPS can maintain the expression of alveolar type II cells, which frequently trans-differentiate into type I cells in other models. These cells are a crucial part of the immune response in the alveoli, and so it is important to model these accurately during testing. As the tissues are more human-relevant, they will also produce more human specific responses to pathogens. Users of our system have determined that using the system allows more sensitive and accurate portrayal of pathogen-host interactions, which allows better differentiation of pathogen types and drug efficacy. Furthermore, the circulating flow in the PhysioMimix system allows the inclusion of circulating immune cells (e.g. PBMCs). This can allow further understanding of lung-immune interactions during infection.
Watch this short COVID-19 presentation from customers at Liverpool School of Tropical Medicine for further insights
Can you include immune cells in your lung-on-a-chip models/pulmonary infection assays?
We can! Thus far, we have done proof of concept studies using cell line monocytes, including them in the perfused media (to mimic circulating monocytes) as well as in the apical side of the alveolar model (to mimic alveolar macrophages). When included in the alveolar epithelium, the cells were seen to differentiate to a macrophage-state and respond to stimuli appropriately through inflammatory signaling and localization to sites of infection. The circulating immune cells can flow around the basolateral side of the well in the perfused media and respond to stimuli through inflammatory signaling, thus changing the state of the overall model health.
If you do not find the answer to your question listed, please contact us

